

07
Jun
Upper Lip Shortening and Lip Rejuvenation
Facial proportions and anatomy
The face is divided into thirds.
- Upper Third from hairline to nose, between eyebrows. The forehead is upper one-third.
- The middle third is from the eyebrows to the base of the nose, where the nose meets the upper lip. The nose is the middle third.
- Lower third from base of nose to bottom of chin. The peri-oral area (upper lip, lower lip, chin) is the lower third.
The lower third of the face is divided into an upper one-third and a lower two-thirds. The upper third includes the upper lip, from base of the nose to where the lips meet or the ‘stomium’. The lower two-thirds is the lower lip from the stomium to the lower part of the chin. The zone where the lips touch is the ‘wet/dry vermilion border’. This is the transition between dry outer vermilion, where we have to apply chapstick and wet mucosal lining within the mouth.
The vertical length of the lower lip is, ideally, twice as large as the upper lip. The magic lower lip to upper lip ratio is 1.5 to 1 to 2 to 1. Although the upper lip is smaller in the vertical dimension, it projects in front of the lower lip on the side view (see below). Upper front incisor teeth should be in front of and touching the lower teeth. This is known as Class I Occlusion. If you look at a profile picture and draw a line from the base of the nose to the crease below the lower lip (sub-labial crease), you will see the difference in projections of the upper and lower lip in front of the line.
Upper Lip Anatomy
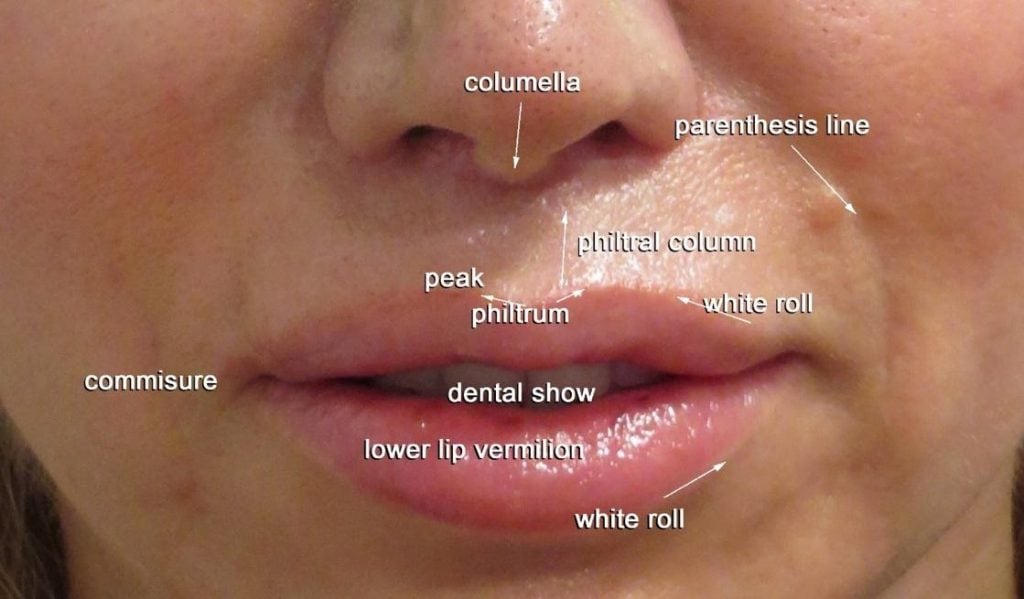
From the front view, the facial skin of the upper lip extends from the base of the nose to the roll at the edge of upper lip vermilion. The upper lip vermilion edge is divided into three, a middle bow and two sides. The middle part has a bow shape known as the Cupid’s bow. At each end of the bow area, a ridge or philtral column, extends vertically to the nose. The hollow in the bow area, between the columns, is the philtrum. The point where the bow meets the column is the peak. On each side of the peak the upper lip edge extends out to the corners of the mouth.
Any enlargement of the upper lip with fat or fillers should consider this anatomy of youth and preserve the ideal relationship of the upper to the lower lip and the three-part structure of the upper lip.
Lower Lip Anatomy
The lower lip consists of two parts or ‘pillows’ that meet in the middle. Between the two pillows there may be a groove or a small depression. Patients often like this midline separation in the lower lip and want to preserve it.
Mouth Width
The width of the mouth is ideally, the distance between two vertical lines dropped from the inner angle of each eye. Julia Roberts has a particularly wide mouth whereas Saoirse Ronan has a more classic width.
Aging
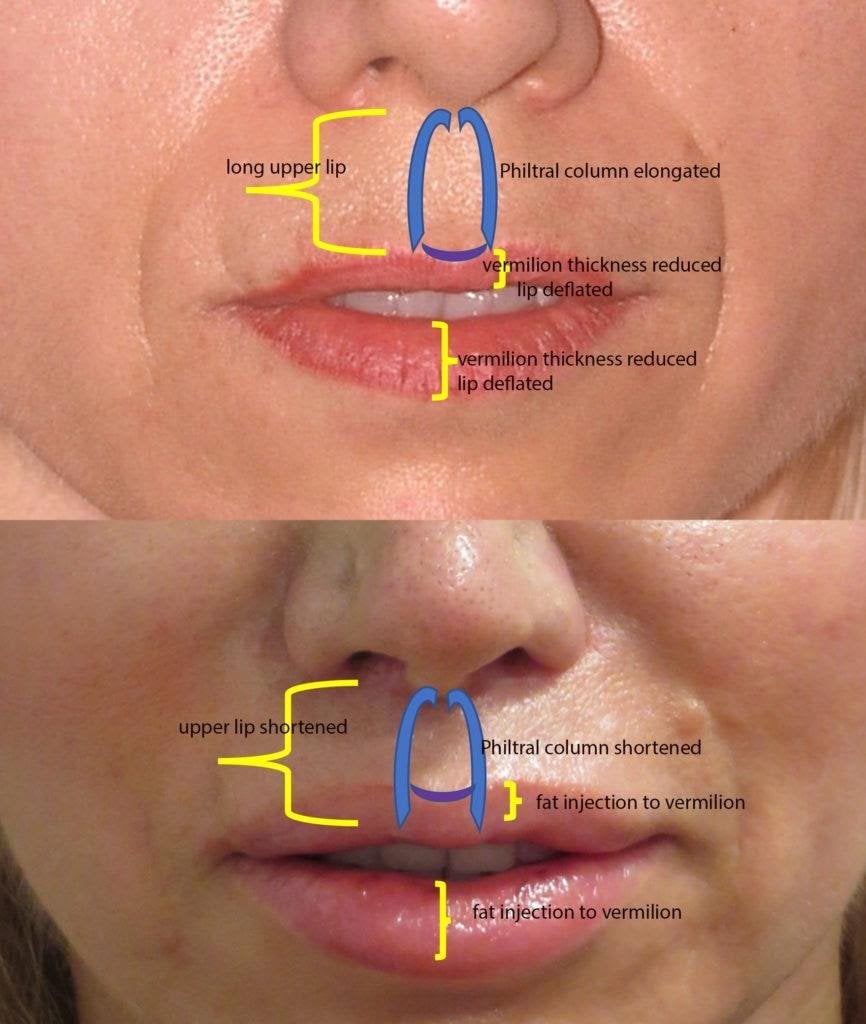
As we age, the upper lip gets longer. It can get quite ‘horsey’ looking. The upper lip is the skin that stretches between the base of the nose and the red part of the upper lip. In contrast, the red part or vermilion, of the upper lip (as well as the lower lip),loses volume and becomes shorter in a vertical dimension. As the upper lip lengthens, the teeth disappear. In the youthful mouth, about 1/8th of an inch of the upper teeth are visible with the lips at rest.
Upper lip skin can be long and lips can be thin, in youth also. If so, facial aesthetics are improved by shortening the upper lip and enlarging the lips. Enlarging the upper lips with filler or fat, without shortening the upper lip, will give the appearance of a shorter upper lip. The larger vermilion makes the upper lip skin proportionally smaller.
With age, there are changes in the nasal tip and the chin. The tip of the nose gets bigger and drops. The result may be a hooked nose. The fat in the chin fat pad loses its projection and its attachments to the jawbone. The chin fat sags resulting in a crease under the chin. This known as the witch’s chin deformity. The combination of a drooping nasal tip, hooked nose, and a witch’s chin, gives the appearance of a fairytale witch in profile.
These additional signs of aging can be corrected with a nasal tip rhinoplasty and a chin augmentation. See below.




The edge of the lip known as the vermilion white roll, can be enhanced. The red part of the lip or vermilion can be filled and plumped. Vermilion white roll injection adds definition to the edge of the lip fills in smoker’s lines. Filling of the vermilion, smooths creases and can increase lip height and projection. When enlarging the lips, the upper lip should not be the same size or larger than, the lower lip. It is a marker of a bad lip injection technique and is one of the reasons why patients are often scared of having their lips injected. Bigger is not always better. Over-projecting white rolls give an unnatural look. Overly plumped lips and a prominent lip roll combined are known as the trout pout. Lips of an equal size start to look like a vagina.
Lip Lift Surgery
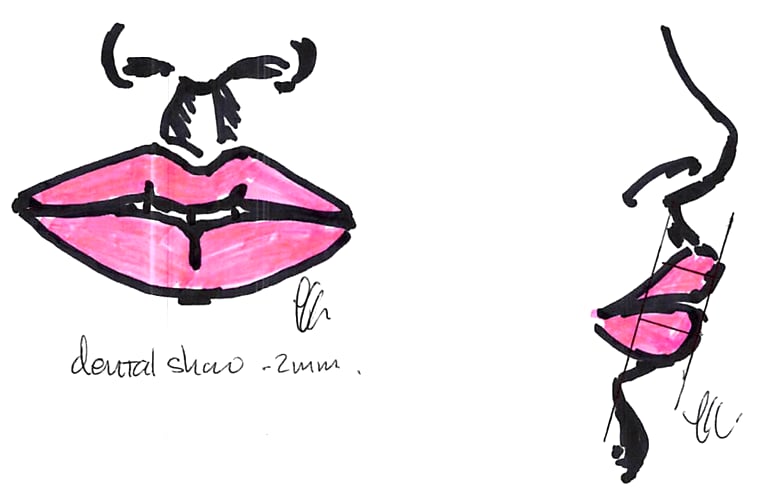
A lip shortening procedure shortens the vertical length of the skin of upper lip and elevates the vermilion white roll. The procedure is done under local anesthesia and takes about 45 minutes. The most important part of the surgical technique is to do the lip shortening first before fat or filler injection to the lips. The skin excision in the upper lip is shaped like a ‘gull wing’, a ‘Texas Long-Horn’ or a crescent and is sited immediately below the nose, where it meets the lip (Figure 3). This is in the crease below the nostril (alar) rim and the columella (Photo 2). The columella is the bridge of skin between the two nostrils. The skin incision may extend into the floor of the nostril to reduce its visibility. After the skin is removed, a small strip of orbicularis oris muscle (the muscle that pinches and puckers the lips) may also be excised. The muscle is then resuspended to the base of the nose so as to give a more durable lift and to further evert the upper lip. It is better to overcorrect to get the best long-term result.

Skin stitches are removed at two to five days to avoid stitch marks. The procedure can also be done in conjunction with nostril narrowing and debulking. A tip rhinoplasty, chin augmentation, and a face-lift can be done together.


Photo 5. [Before and after upper lip shortening, fat injection to lips, nasal tip plasty and chin implant.]
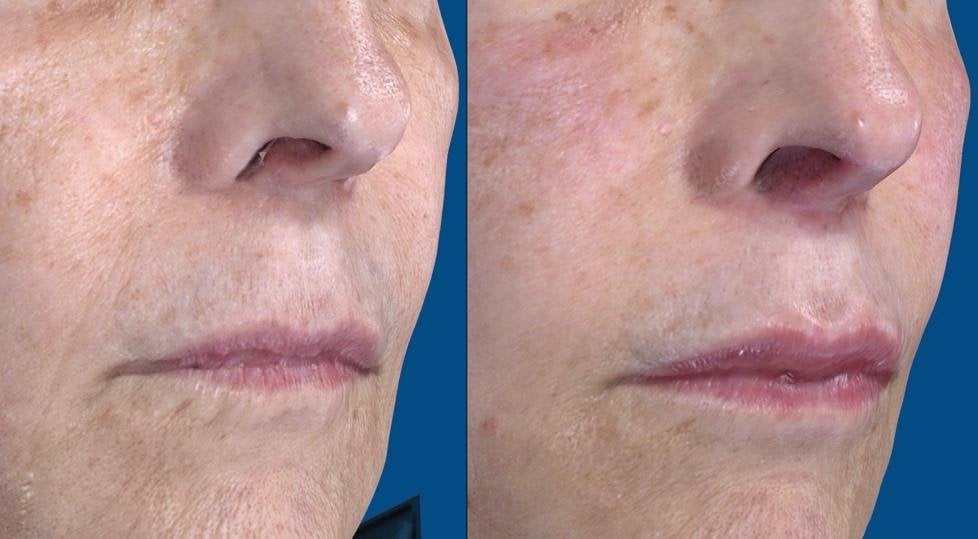


Photo 6. [67-year-old 5 months after surgery. This patient did not want lip injection or a greater lip lift. It is important to overcorrect and remove at least 6 mm from the upper lip. A portion of the orbicularis muscle, under the nose, can also be removed to increase the effect of the lip lift. The scar can be placed into the floor of the nostril but in cases where there is a well-developed roll or sill in the floor, the scar should be placed just below, to avoid distorting the natural anatomy.]
The Lip Flip
The Lip Flip is a series of Botox injections into the superficial part of the orbicularis oris muscle. This muscle compresses and puckers the lips. The injections are usually placed in the upper lip at the margin, although they can also be injected along the lower lip margin. Like all Botox injections, they take 3-5 days to take effect. The Lip Flip is often performed at the same time as a Fat or Filler injections to the lips. Commonly used Fillers are Vollure, Juvéderm Ultra-Plus, Juvéderm Ultra and Volbella. The Filler is injected along the vermilion white roll margin to evert the edge of the lip and can also be injected into the red body of the lip or vermilion to increase the volume of the upper and lower lips.




Call Our Office For More Information
Share this Article

Dr. Laurence Kirwan
Dr. Laurence Kirwan, MD, FRCS, FACS, is an internationally renowned, board-certified plastic surgeon with over 30 years of experience. He trained at Manchester University and completed his Plastic Surgery residency at the University of Missouri. A Fellow of the Royal College of Surgeons and American College of Surgeons, he is a leader in aesthetic surgery, specializing in face, breast, and body procedures. Dr. Kirwan has authored multiple scientific papers and books and served as an instructor in prestigious programs. Recognized by Tatler and Russian Vogue, he practices in Connecticut, where he continues to offer personalized, top-tier care to his patients.